
Angioplasty / Stent / Atherectomy
Treatments
What is angioplasty and stenting?
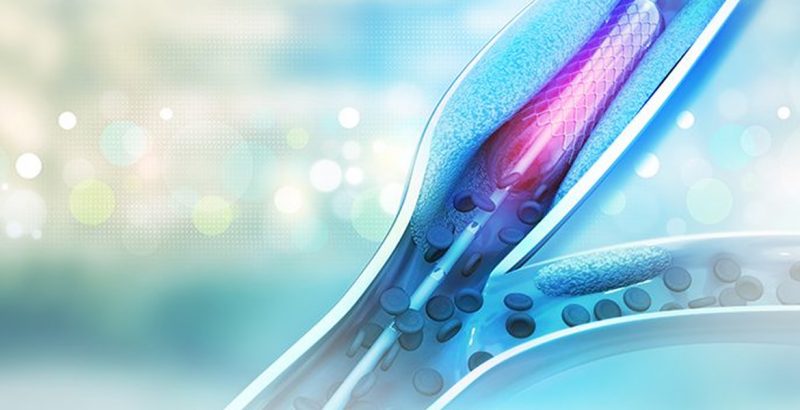
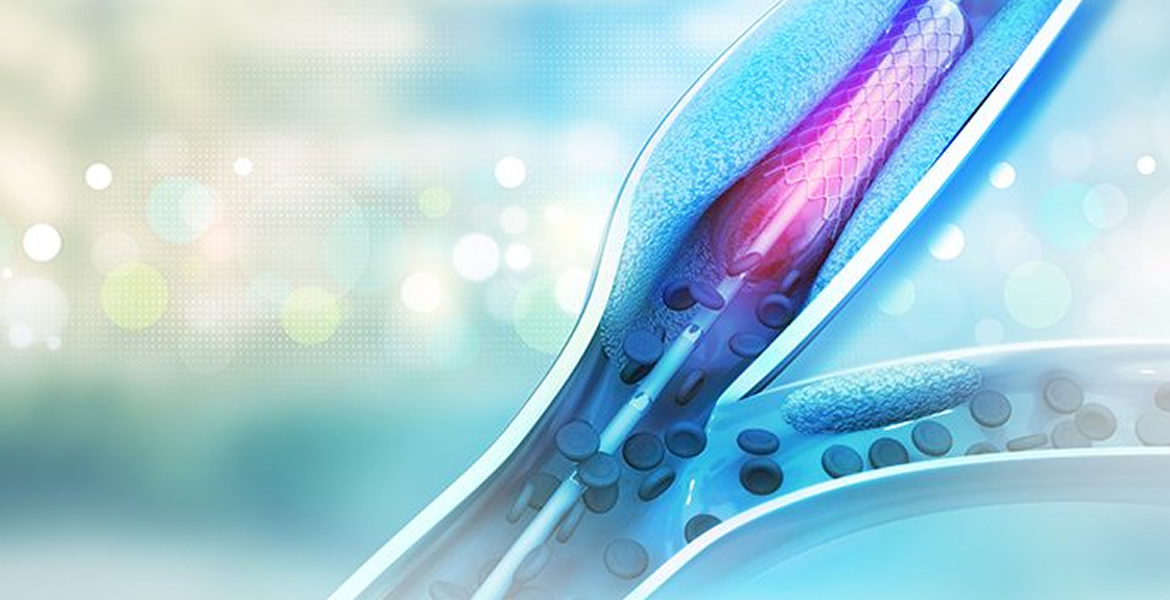
During an angioplasty, your vascular surgeon inflates a small balloon inside a narrowed blood vessel. The balloon helps to widen your blood vessel and improve blood flow. After widening the vessel with angioplasty, your vascular surgeon sometimes inserts a stent depending upon the circumstances. Stents are tiny metal mesh tubes that support your artery walls to keep your vessels wide open.
Angioplasty and stenting are usually done through a small puncture, or sometimes a small incision, in your skin, called the access site. Your vascular surgeon inserts a long, thin tube called a catheter through this access site. Using X-ray guidance, your physician then guides the catheter through your blood vessels to the blocked area. The tip of the catheter carries the angioplasty balloon or stent.
Angioplasty most often is used to treat peripheral arterial disease (PAD), which is another name for hardening of the arteries supplying blood to your limbs or to organs in your body other than your heart. Angioplasty can also be used, in some circumstances, to treat narrowed areas in your veins, which are blood vessels that drain blood out of your limbs or organs and return the blood to your lungs and heart.
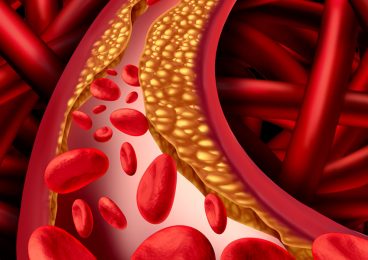
Your arteries are normally smooth and unobstructed on the inside, but as you age, plaque can build up in the walls of your arteries. Cholesterol, calcium, and fibrous tissue make up this plaque. As more plaque builds up, your arteries can narrow and stiffen. This process is called atherosclerosis, or hardening of the arteries. Eventually, enough plaque builds up to reduce blood flow through your arteries causing pain or damage to the part of the body that the artery supplies.
Depending upon the particular circumstances, your physician may recommend angioplasty as an alternative to bypass surgery, which also treats narrowed arteries. For certain types of blockages, angioplasty has some advantages when compared to bypass surgery. For example, angioplasty does not require a large incision. Because of this, angioplasty patients usually spend less time in the hospital and recover at home faster than bypass surgery patients. Also, your physician can usually perform angioplasty while you are awake, whereas bypass surgery requires general or regional anesthesia. Nevertheless, in some circumstances, especially for extensive PAD, bypass surgery may be a better option. Your vascular surgeon will help you decide what alternative is best for your particular situation.
How do I prepare?
First your physician asks you questions about your general health, medical history, and symptoms. In addition, your physician conducts a physical exam. Together these are known as a patient history and exam. As part of your history and exam, your physician will ask you if you smoke or have high blood pressure. Your physician will also want to know when and how often your symptoms occur, and their location.
Next, your physician will order tests to show how much plaque has built up in your arteries. These tests can help your physician determine whether you need an angioplasty or some other form of treatment. The choice of test depends on the blood vessel in question and not all of the tests need to be used for every situation.
These tests may include:
- Pulse volume recordings (PVRs)
- Duplex ultrasound
- Magnetic resonance angiography (MRA)
- Computed tomography (CT) scan
If these tests show that your arteries are moderately to severely narrowed, your vascular surgeon may also plan a test called angiography. An angiogram directly shows your blood vessels on an X-ray and may also provide an opportunity to treat the narrowing with angioplasty at the time of the angiogram. During angiography, your vascular surgeon inserts a long, thin tube called a catheter into an artery in your groin or arm after first making the area numb with a local anesthetic. Using X-ray guidance, your physician then guides the catheter through your blood vessels to the blocked area and injects a dye that allows the arteries to be seen on the X-ray. The dye is later eliminated in your urine after it is filtered out by your kidneys.
Your vascular surgeon will give you the necessary instructions you need to follow before the procedure, such as fasting. Usually, your vascular surgeon will ask you not to eat or drink anything several hours before your procedure. Your vascular surgeon will discuss with you whether to reduce or stop any medications that might increase your risk of bleeding or other complications. If you have any allergies to contrast dye, which is used in angiography, you should tell your vascular surgeon at this time. Since the contrast dye may contain iodine, you should also let your vascular surgeon know if you have allergies to iodine or shellfish.
Before your procedure, your physician may order tests to check your kidney function as well as your blood’s ability to clot. In addition, he or she may insert an IV to deliver fluids. Depending upon the circumstances, the angioplasty procedure may sometimes be performed at the time of the initial angiogram or later on as a separate procedure.
Am I a candidate for angioplasty and stenting?
You may be a candidate for angioplasty and stenting if you have moderate to severe narrowing or blockage in one or more of your blood vessels. Usually, you will also have symptoms of artery disease, such as pain or ulceration, in one of your limbs.
If you have extremely hard plaque deposits, blockages that contain blood clots or a large amount of calcium, extensive or particularly long blockages, blood vessel spasms that don’t go away, or complete blockages that cannot be crossed with the catheter, you probably are not a good candidate for angioplasty.
Am I at risk for complications during angioplasty and stenting?
Complications to angioplasty and stenting may include reactions to the contrast dye, weakening of the artery wall, bleeding at the access puncture site in the vessel or the angioplasty site, re-blocking of the treated artery, and kidney problems. Additionally, blockages can develop in the arteries downstream from the plaque if plaque particles break free during the angioplasty procedure. If severe, these can lead to worsening of the blood flow.
If you have diabetes or kidney disease, you may have a higher risk of complications from the contrast dye, such as kidney failure. In the case of kidney disease, sometimes pre-treatment with medications or fluids may decrease the impact on your kidneys.
People with blood clotting disorders also may have a higher risk of complications from the procedure. If the plaque deposits in your arteries are especially long, you may have a greater chance of your artery closing up again after angioplasty and stenting.
What happens during angioplasty and stenting?
Your physician will usually insert the angioplasty catheter through a small puncture point over an artery in your groin, your wrist, or your elbow. Before the insertion, he or she will clean your skin and shave any hair in the immediate area. This is done to reduce your risk of infection. Your physician numbs your skin and then makes a small cut or puncture to reach the artery below. Although you may be given some mild sedation, your vascular surgeon will usually want you to stay reasonably alert to follow instructions and describe your sensations during the procedure.
Your vascular surgeon then inserts a guide wire or a guide catheter into your artery. Using a type of x ray that projects moving pictures on a screen, your physician guides the catheter through your blood vessels. Because you have no nerve endings in your arteries, you will not feel the catheters as they move through your body.
Next, your vascular surgeon will insert a balloon catheter over the guide wire or through the guide catheter. The balloon catheter carries a deflated and folded balloon on its tip. Your vascular surgeon guides the balloon catheter to the narrowed section of your artery. He or she partially inflates the balloon by sending fluid through the balloon catheter.
Your vascular surgeon watches the x ray screen for signs of a pinch in the balloon. Then, your vascular surgeon will inflate the balloon more, until the pinch caused by your artery flattens out. When the balloon is full, your vascular surgeon may deflate and re-inflate it repeatedly to press the plaque against your artery walls. Usually, this process takes a few minutes. Sometimes, if you have a severe blockage, your physician may need to inflate and deflate the balloon longer.
Your artery may stretch and your blood flow through the artery stops when the balloon is pushing your artery open. This may cause pain. However, the pain should go away when your vascular surgeon deflates the balloon and normal blood flow resumes. Make sure to tell your physician if you experience any symptoms during angioplasty.
There is a risk that your artery will re-narrow or become blocked again at the site where the balloon was inflated. This can happen soon after the procedure, or months to years later. Re-narrowing of your artery is called restenosis, and if your artery suddenly becomes blocked again it is called re-occlusion. Restenosis can happen when scar tissue builds up inside your arteries where the balloon compressed your plaque deposits.
After angioplasty, your vascular surgeon will sometimes need to use a stent to brace the artery open to prevent re-occlusion. A stent is a tiny mesh tube that looks like a small spring, and comes in a variety of sizes. To place a stent, your physician removes the angioplasty balloon catheter and inserts a new catheter. On this catheter, a closed stent surrounds a deflated balloon. Your vascular surgeon guides the stent through your blood vessels to the place where the angioplasty balloon widened your artery. Your physician inflates the balloon inside of the stent. This expands the stent. Your physician then deflates and removes the balloon. The stent remains in place to support the walls of your artery. Your artery walls grow over the stent, preventing it from moving. Although stents help prop open your arteries, scar tissue sometimes can eventually form around stents and cause restenosis.
Once your vascular surgeon finishes angioplasty and stenting, he or she removes all of the catheters from your body. If blood-thinning medications have been used, your physician may leave a short tube, called a sheath, in your artery for a short time until the medications have worn off sufficiently to allow the puncture site to seal over when the sheath is removed.
Eventually, your physician removes the sheath and presses on the puncture area for 15 to 30 minutes to prevent bleeding. Sometimes, instead of pressing, your physician may close the area with a device that functions like a tiny cork, or he or she may use stitches.
Angioplasty and stenting usually takes between 45 minutes and 3 hours, but sometimes longer depending upon the particular circumstances.
What can I expect after angioplasty and stenting?
Usually, you will stay in bed for six hours after your angioplasty. During this time, your vascular surgeon and the hospital staff closely monitor you for any complications. If your physician inserted the catheters through an artery in your groin, you may have to hold your leg straight for several hours. Similarly, if your arm was used, then you will need to hold it still to minimize the risk of bleeding.
If you notice any unusual symptoms after your procedure, you should tell your vascular surgeon immediately. These symptoms include leg pain that lingers or gets worse, a fever, shortness of breath, an arm or a leg that turns blue or feels cold, and problems around your access site, such as bleeding, swelling, pain, or numbness.
After you return home, your vascular surgeon will give you instructions about everyday tasks. For example, you should not lift more than about 10 pounds for the first few days after your procedure. You should drink plenty of water for 2 days to help flush the contrast dye out of your body. You can usually shower 24 hours after your procedure, but you should avoid baths for a few days.
Your physician may prescribe aspirin or other medications that thin your blood. These medications will help prevent clots from forming on your stent. Your physician may also ask you to follow an easy exercise program, like walking.
You will be asked to schedule a time to see your physician after the procedure. At this appointment, your physician may check your blood to make sure your medications are at the right dosage. He or she may also use tests to see how blood is flowing through your treated artery.
Are there any complications?
Serious complications are unusual following angioplasty and stenting but, nevertheless, can occur.
Less serious complications include bleeding or bruising where your vascular surgeon inserted the catheters. Sometimes, the hole created by the catheter does not completely close. This can create a false channel of blood flow. Rarely, an abnormal connection can form between an artery and a vein at the place where the catheter was inserted. These problems usually go away. However, if you have any serious symptoms, your vascular surgeon can treat you.
You may have an increased risk for blood clots forming along your stent, especially in the first month after your procedure. To reduce this risk, your physician may prescribe medications that thin your blood.
As more time passes after your angioplasty and stenting, restenosis becomes more likely. Stents, especially drug-coated stents, may reduce this risk. However, in some cases, you may need a repeat angioplasty or a bypass surgery if a restenosis develops.
Serious, but unusual complications include:
- Reaction to contrast dye
- A clot in the artery that your physician treated
- A torn or weakened blood vessel
- A large blood collection called a hematoma
- Kidney problems
- Damage to the lining of the artery (called dissection)
- Blockages developing in arteries downstream from the treated artery from particles of the plaque breaking free (called embolization).
Related Conditions
Related Symptoms




- Contact Us Today: 210.237.4444
- Veintec: 210.483.8822







TOS/Privacy Policy | Notice of Nondiscrimination | Aviso de no Discriminación
© 2024 Peripheral Vascular Associates - San Antonio. All Rights Reserved.
San Antonio Website Design & Development - Backyard Studios
© 2024 Peripheral Vascular Associates - San Antonio. All Rights Reserved.
San Antonio Website Design & Development - Backyard Studios